
- Downloads:
- Flowchart for Sarawak Antenatal VTE Risk Assessment (Admission)
- Flowchart for Sarawak Postnatal VTE risk Assessment (Discharge)
- Sarawak Home Visit Venous Thromboembolism Checklist Antenatal and Postnatal
- Sarawak Venous Thromboembolism Risk Assessment Checklist For hospitalised Patients (Antenatal and Postnatal)
VenousThromboEmbolism Risk Factors:
ANTENATAL:
- Previous VTE (estrogen related, unprovoked or recurrent) [3]
- Previous VTE (provoked, eg accident) [2]
- Thrombophilia [2]
- Medical illness (SLE, Cardiac, Connective tissue, Renal disease, Malignancy) [2]
- Family history of VTE [1]
- Age >35 years [1]
- Parity of 5 or more [1]
- Obesity (BMI>40kg/m2) [2]
- Obesity (BMI>30kg/m2) [1]
- Gross varicose veins [1]
- Smoker/ IVDU [1]
- Multiple pregnancy [1]
CURRENT EVENTS OR ADMISSION:
- Hyperemesis Gravidarum requiring admission [1]
- Pre-eclampsia [1]
- Dehydration/ Ovarian Hyperstimulation Syndrome (complication of fertility Rx)
- Hospital stay / immobilization > 3days [1]
- Systemic infection (eg active TB, pneumonia) [1]
- Chorioamnionitis [1]
- Surgery in pregnancy or puerperal period (this includes BTL within 42 days of delivery but excluding ERPOC & minor Toilet & suture) [1]
- Long distance travel by road/air travel > 8 hours non stop [1]
DELIVERY (CURRENT PREGNANCY):
- Caesarean section (emergency & elective) [2]
- Instrumental delivery [1]
- PPH > 1.5 L [1]
- Prolonged labour > 24 hours [1]
- Third/fourth degree perineal tear [1]
- Vulvo/vaginal haematoma [1]
- Septic miscarriage/ Molar pregnancy [1]
This assessment should be performed at:
- During each hospital admission
- Post delivery before discharge
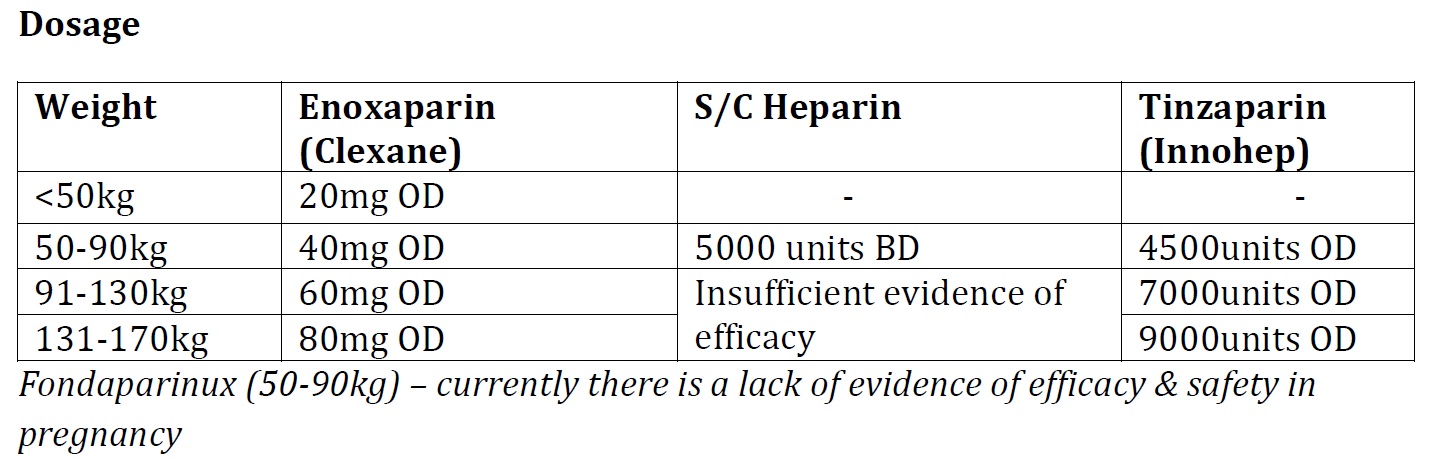
Patient’s who should be given thromboprophylaxis:
- ANTENATALLY – score > 3 (duration of thromboprophylaxis to be decided or discussed with an O&G specialist)
- POSTNATALLY – score > 2 (Rx duration of at least 1 week)
General advice
- Antenatal patients with score of > 3 will automatically be CODED YELLOW
- Postnatal patients with a score of > 2 will be CODED YELLOW
- Initiation of thromboprophylaxis can be given in any hospital or clinic with supply of LMWH/Heparin. Patients to be counselled and trained to administer LMWH by themselves at home. For s/c Heparin, it needs to be given in a hospital setting as an inpatient or outpatient.
- Subsequent supply for LMWH for patients requiring long term treatment to be arranged at nearest hospital or health clinics for patient’s convenience.
- Upon discharge, all cases requiring thromboprophylaxis should have a ‘High Risk E–Discharge’ and home visits by community nurse within 7 days of discharge.
- All antenatal patients and up to 6 weeks postnatal should be advised to drink adequate amounts of fluids and ambulate.
- All patients should be counselled on the signs and symptoms’ of DVT and PE such as calf pain, calf swelling or redness, shortness of breath, chest pain or fever. Such patients should seek immediate attention at the nearest clinic.
- For patients in remote areas or if in doubt, refer to a medical officer, FMS or an O&G specialist